
Causes of headache
Headaches are a very common problem; up to 3 in every 4 adults suffer from at least one each year. Often these are mild, short-lived, and require no treatment. Others can be debilitating, and a few need urgent intervention to prevent disability and death. Knowing about the causes helps guide history-taking, examination, and tests that can reveal the problem and guide care. It is a surprisingly large topic, so while I’ve tried to touch on many key diagnoses, be aware that others exist!
Primary headaches
Headaches that are not the result of another condition.
Patterns of pain in primary headache. If you’d like a poster, I’ve got this and secondary causes of headache in a PDF bundle here.
Migraine headache

Migraine is a common disabling hemicranial (one-sided) severe headache which may occur with or without an ‘aura’. An aura is one or more fully reversible symptom of the central nervous system including (but not limited to):
visual changes
numbness
weakness
difficulty speaking
balancing
An aura develops gradually over 5 minutes or more, and resolves fully within an hour. The headache causes one-sided pain associated with sensitivity to light, noise, and nausea/vomiting. Typically they last 4-72 hours. The headache of a typical migraine can arrive with an aura, after one, or not happen at all for some luckier people.
Tension headache
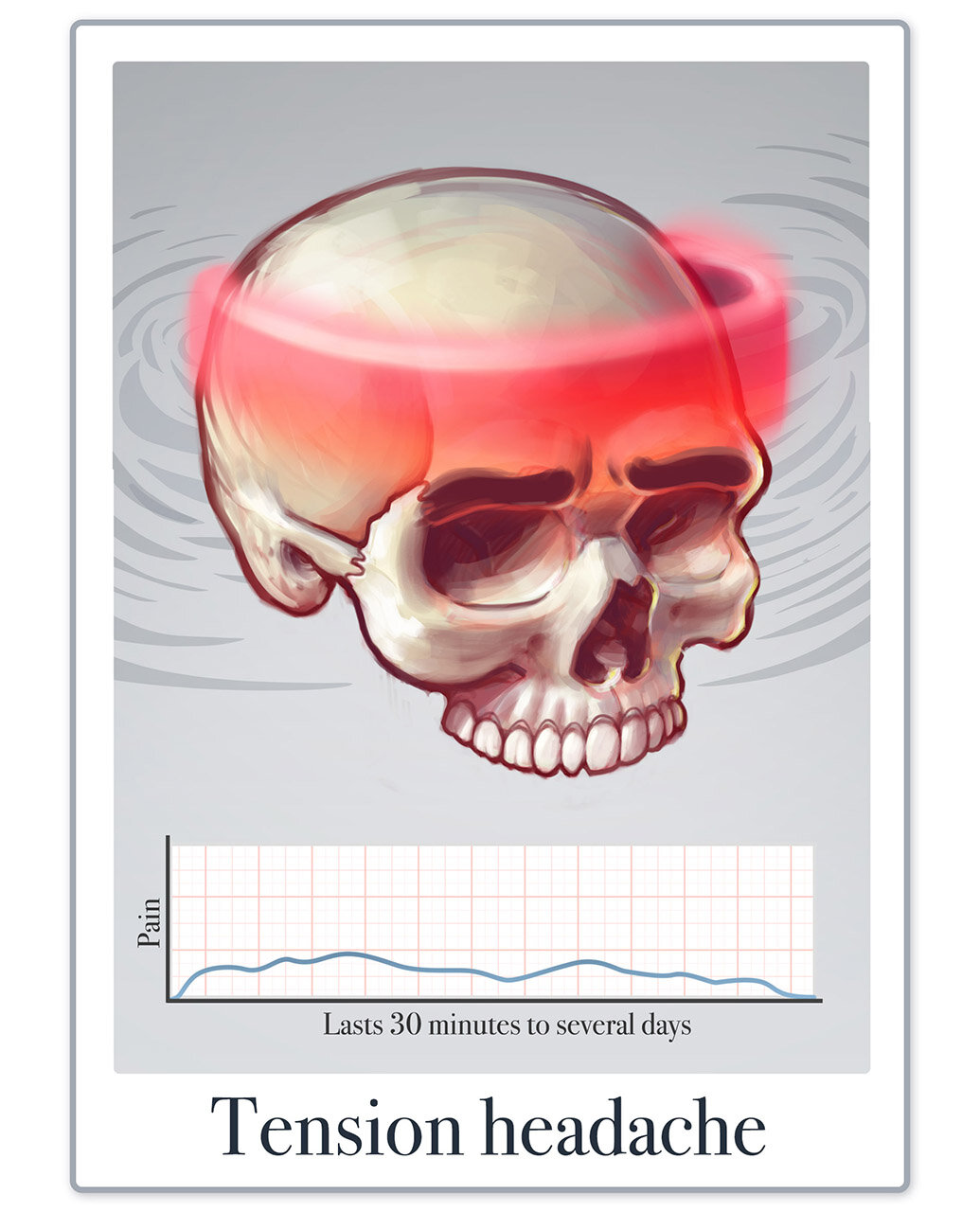
Tension headaches are very common and cause mild to moderate pain and tenderness around the head and neck, lasting minutes to days. The pain is often described as ‘band-like’ above the eyebrows, sometimes encircling the head like a cap. People are usually able to continue daily activities through the discomfort, but the pain can be quite disabling when recurring or long lasting. When a person has tension headaches on 15 days or more per month they are called ‘chronic tension headache’.
Cluster headache

Attacks of severe pain around one eye, lasting 15 mins to 3 hours, occurring 1 to 8 times per day, and a severe feeling of restlessness/agitation. Other features occur on the same side as the pain and may include a constricted pupil, eye redness, eyelid swelling and drop, nasal congestion, a runny nose, and facial sweating.
Secondary headaches
The bulk of the topic of headaches lies in secondary causes, that is, headaches that are a result of another problem.
Secondary causes of headache, an illustrated differential diagnosis. If you’d like to print your own you can get a copy here.
Trauma to the head and neck
If structures in the head and neck are injured, they can hurt. E.g ‘whiplash’ or a concussion sustained in a road traffic collision. Hopefully this one is obvious.
Vascular disorders
Ischemia
This refers to the blood supply being restricted or cut off e.g. during a stroke
Inflammation
In temporal arteritis, the temporal artery becomes inflamed in patches. This can result in permanent vision loss without prompt treatment. Other symptoms include jaw pain, vision loss, fever and fatigue.

Bleeding
If the blood vessels supplying the brain bleed, problems arise from:
tissue not receiving enough blood to survive
increasing pressure in the fixed bony box of the skull, squishing softer important things like the brain, blood vessels, and nerves
A bleed between the meninges (membrane layers covering the brain) can quickly become a medical emergency. Other things that bleed include a malformation of the blood vessels, and ruptured aneurysms. Unruptured aneurysms can cause headache as they grown from the ‘mass effect’ they cause pressing on other structures.

Intervention
Fixing one problem can cause another, such as a craniectomy to remove a part of the skull to reach a brain tumour, or placing a stent in an artery to improve blood flow to the brain.
Clot
When blood clots inside a vessel it disrupts the normal blood flow to (e.g. an ischaemic stroke) or away from brain tissue (e.g. sinus vein thrombosis).

Cerebrospinal fluid
The brain is bathed in a clear liquid called the cerebrospinal fluid (CSF). This provides nutrients, takes away waste materials, and helps cushion the brain from impact. If the flow of CSF is affected by a blockage or leak, this raises or lowers the CSF pressure, both of which can cause headache.
Sometimes doctors can cause a small leak when taking a sample of CSF to help investigate other problems. This can cause a headache from low CSF pressure, which is much worse on sitting or standing as the brain sags within the skull. It usually self-resolves but an ongoing leak is sometimes treated with a ‘blood patch’ where a patient’s own blood is injected at the site of the leak to form a ‘patch’.
Blocked CSF flow can be caused by mass effect such as a tumour, or may be a problem from birth resulting in hydrocephalus. A ‘shunt’ is a small tube which can treat the latter by diverting CSF to another location e.g. from a brain ventricle to the abdomen where it is absorbed.
Intracranial neoplasm/tumour
The brain itself doesn’t have pain receptors, but tumours cause problems by their ‘mass effect’ as they squish nearby structures such as nerves and blood vessels, and may block CSF flow.
After a seizure
Headache is common following a seizure in what is called the ‘post-ictal’ period. These usually last less than six hours if they occur.

Substance use or withdrawal
Headache is a common side effect of many drugs, both those used medicinally (e.g. painkillers) and recreationally (e.g. caffeine, alcohol, and cocaine). Many ‘painkiller’ medicines cause headache when used regularly for weeks or months (chronically), e.g. to treat recurring headaches. In this case, the solution (oddly, you might think) is often to stop taking the pain relief. Headache is also a common side effect when withdrawing from substances like alcohol and heroin.

Infection
Headache is a common symptom of infections. The most concerning cause to rule out is probably meningitis (infection of the meninges - the brain and spinal cord covering) and septicaemia (infection of the blood); two related problems which can maim and kill in a matter of hours.
Meningitis headaches can be worsened by looking down, touching the chin to the chest, as this stretches the meninges. It is associated with fever, sweats, sensitivity to light, nausea and vomiting, a non-blanching rash (doesn’t fade when pressed with and viewed through a glass). As the disease progresses, people become confused, drowsy, fall unconscious, may have seizures, and die. It’s scary stuff and worth considering early.
For those who live in, or have recently travelled to endemic areas, mosquito-borne diseases like Chikungunya should be considered.
Shingles
After a person has been infected with chicken-pox, the virus responsible (herpes varicella-zoster) climbs up a nerve that supplies a patch of skin. Here it may lay dormant forever more. For some unfortunate individuals however, it returns as a blistering, painful rash called shingles which affects the patch of skin that nerve is responsible for. The pain is often described as burning or throbbing. This can be very uncomfortable on the face and may threaten vision or hearing when the eye or ear is involved. Sometimes the nerve pain remains after shingles resolves; this is called post-herpetic neuralgia.

Disorder of homeostasis
In order to function, every cell in our bodies must maintain a delicate balance in their internal environment in order to carry out their jobs. This is called ‘homeostasis’. Too much, or too little of a substance like oxygen or glucose (sugar) can wreak havoc on normal function. This can be driven by a problem in the external environment (e.g. lack of oxygen at high altitude, or from carbon monoxide poisoning), or the internal environment (e.g. thyroid problems changing the bodies metabolism, or massive shifts in blood chemicals during dialysis). Behaviour also plays a role, such as when fasting or eating a high-sugar diet.

Referred pain
Pain in any structure of the head and neck can radiate to cause a headache. Think about the eyes (e.g. strain from the wrong glasses prescription), ears (e.g. a burst eardrum), nose (e.g. sinus problems), teeth (e.g. a cavity or abscess), jaw (e.g. tempero-mandibular joint dysfunction), and neck (e.g. a trapped nerve).
Mental health
The brain is a powerful organ; mental health issues such as depression and anxiety can manifest physical symptoms like nausea, fatigue, and headache. This process is called somatisation. Headache may also be experienced in a psychotic illness.
Fin
And that’s it! My differential isn’t exhaustive (despite how tiring it may be to read) but should give you a good flavour for many common and important causes of headache. Can you think of any others worth touching upon? To read deeper into the nitty-gritty of diagnosing headache, check out the International Classification of Headache Disorders (ICHD), a fantastic resource which can be found here: https://ichd-3.org/
This art is part of my “Medical Mentalism” series, an independent effort fuelled by coffee from my Patrons. If you’d like to send some my way click here, or consider sending a regular cup via the Scrub Club on Patreon - thank you to all who help keep me going!